
3.4 Injecting SC Medication Via an Insuflon
Download Word version
Download PDF version
The information provided in the following sections is intended to guide safe practice in the POGO Satellite Program. It is not intended to replace your institutional policies and procedures. Please ensure all staff are aware of their own institutional policies and procedures and refer to them as their primary source.
This procedure is a controlled act authorized to Nursing. If you infrequently practice this procedure, please refer to “Decision Tree” from the College of Nurses of Ontario (CNO) for performance of procedures to help you decide whether or not you should perform the procedure.
Introduction
The purpose of this section is to provide guidance when inserting, administering medication through and removing an Insuflon indwelling subcutaneous catheter.
Use of the Insuflon
The Insuflon can be used with subcutaneous medications such as Granulocyte Colony-Stimulating Factor (G-CSF). Only 1 medication is to be administered per Insuflon subcutaneous catheter.
Equipment
The Insuflon catheter is for subcutaneous injection. The catheter is made of Teflon with a silicone membrane covering the injection hub. No other extensions, connections or other tubing (i.e., T-piece) should be added to the device.
The dressing that accompanies the Insuflon catheter has a clear window to allow visualization of the insertion site, and an open section to allow access to the hub.
Note: The dead space in the catheter is less than 0.0075 ml. If more than 10% of the medication is lost in the catheter’s dead space volume of 0.0075 ml, consult the physician and pharmacy before using the Insuflon. A small amount of compatible solution may be considered to flush the medication if necessary.
Timing
The catheter must be changed every 7 days or sooner if there are any signs of redness, pain, swelling, exudate or bleeding at the site or difficulty injecting.
Procedure: Insertion
Equipment
- 1 Insuflon catheter with dressing
- 1 antiseptic skin cleanser
- Topical anesthetic or patch
| Key Steps | Rationale |
| Assemble the equipment and then wash your hands. | Hand hygiene. |
| Select an insertion site. Avoid skin folds or lines of clothes. | Choices are the posterior aspect of the upper arm, anterior upper thigh or abdomen above the umbilical area. Placement in the limb should be vertical, pointing upwards toward the head. This facilitates easier access during administration of the medication. Placement in the abdomen should be horizontal, towards the umbilicus. |
| Apply topical anesthetic to site as needed. | Apply topical anesthetic to site as prescribed before insertion to minimize discomfort associated with needle insertion. |
| Clean the selected site with an antiseptic cleanser and allow to dry for 1 minute. | Antiseptic skin cleansers remove surface bacteria. The skin should be dry to ensure secure adhesion of dressing. |
| Open package just before use by pulling the paper lid from the plastic package. | The Insuflon is sterile if the package is undamaged. Check the package and the expiry date. Do not use the Insuflon if the package is already opened or damaged or the expiry date has passed. |
| Hold the catheter hub and remove the protection cap. Place the cap in the rear of the grip. | During insertion, hold the Insuflon hub between the thumb and index finger. |
| Support the patient securely with one hand and pinch the skin at the site of insertion. Insert the Insuflon subcutaneously into the fatty tissue as far as possible at a 20˚ to 45˚ angle in one smooth quick movement with the bevel up. | You may require an assistant(s) to stabilize the child’s limb. The Insuflon should be inserted deep into the subcutaneous tissue; the angle will depend on the size of the patient. Some medications can be locally irritating if the Insuflon is inserted too superficially. If Insuflon insertion is too slowly, there is a risk of the catheter peeling back from the needle. 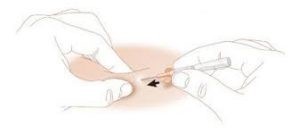 |
| Remove the needle by holding the catheter hub firmly and pulling the needle out slowly. Dispose of the needle in a Sharps container. | Do not withdraw the catheter during placement. Use a new Insuflon if the catheter is damaged or withdrawn. Do not reinsert the needle. |
| Secure Insuflon by applying the dressing provided from the catheter end first, ensuring the insertion site is clearly visible through the clear plastic window and the hub is left open to air. | Completely adhere dressing to skin to prevent pathogens from entering the insertion site. Tegaderm may be applied over the Insuflon and dressing to enhance the stability of the dressing, so long as access to the hub is not obstructed.  |
| Document the insertion procedure in the patient record. | Include location of placement, any problems encountered and patient response to procedure. |
| The insertion site must be observed daily for signs of redness, swelling, exudate and bleeding and documented in the patient record. | If the site becomes inflamed or infected, remove the Insuflon and place a new one in a new site if still needed. |
Procedure: Injecting Medication
Equipment
- Medication to be injected, drawn into syringe
- 27 gauge or smaller needle, length 5mm to 10.5mm, attached to medication syringe
- Antiseptic cleanser
| Key Steps | Rationale |
| Assemble the equipment and then wash your hands. | Hand hygiene. |
| Identify patient and check medication. Explain procedure and prepare patient and family as necessary. | Ensure right drug is being administered to the right patient by the right route. |
| Assess the site and dressing. | The insertion site must be observed daily for signs of redness, swelling, exudate or bleeding and observations documented daily. |
| Cleanse injection cap with antiseptic swab and allow for drying time. | Removes surface bacteria. |
| Gently insert needle straight into the injection hub through the silicone membrane, rotating the syringe gently as it is advanced. Do not use excessive force to insert the needle. | Angle of the syringe needle may need to be adjusted and/or rotated gently to aid insertion. View image 3.4 Inject Medication via Insuflon The needle must penetrate the silicone membrane by at least 3mm and no more than 10mm. Rotating the needle helps to move it away from the inner wall of the hub. |
| Instill the medication slowly, then remove the needle from the hub. | Slow injection helps to reduce irritation caused by the medication. |
| Document the medication administration and condition of site. |
Procedure: Removal
| Key Steps | Rationale |
| To remove the Insuflon, carefully peel off the dressing beginning at the catheter end and remove catheter. | Never exceed 7 days indwelling time. If the Insuflon is to be removed post administration of medication, a minimum of 15–30 minutes should elapse prior to removal to allow for optimal medication absorption. Remove the catheter early if there is any pain, swelling or firm tissue, leakage or loose dressing. Place a new Insuflon in a new site, if still needed. Discard Insuflon after removal in appropriate biohazard garbage container. |
| It is recommended to place the new Insuflon before removing the old one to ensure rotation of sites. | Rotate insertion sites to avoid tissue damage and the formation of lipo-hypertrophies. |
| Document the procedure in the patient record. Include where the Insuflon was placed. | To ensure that the catheter does not exceed 7 days indwelling time. |
This guidance document was developed by Ms. Lisa Egan-Bates, Southlake Regional Health Centre, Newmarket, Mr. Kaniska Young Tai, The Hospital for Sick Children, Toronto and Ms. Sylvie Kozlowskyj, Northeast Cancer Centre, Health Sciences North, Sudbury. Reviewed in consultation with Ms. Kirsty Morelli, Scarborough Health Network, Centenary Hospital and Ms. Christina McCauley, POGO/The Hospital for Sick Children, based on the sources below.
References
- Insuflon® Instructions for Use. Unomedical Denmark. infusion-set.com. Revised from Provincial Pediatric Oncology Satellite Program: A Blueprint for Service. Version 4. February 2008. J. INJECTING SC MEDICATION VIA INSUFLON®.
- The Royal Children’s Hospital, Nursing Clinical Guidelines (2014). Subcutaneous Catheter devices management of Insuflon™ and BD Saf-T-Intima Devices. Retrieved November 5, 2020 from https://www.rch.org.au/rchcpg/hospital_clinical_guideline_index/Subcutaneous_catheter_devices_management_of_insuflon_and_BD_safTIntima_devices/.
- Winnipeg Regional Heath Authority Palliative Care Program (2010). Procedure for Subcutaneous Insertion, Removal, Medication Administration and Fluid Administration for Community Palliative Care Patients. Retrieved November 5, 2020 from https://www.virtualhospice.ca/Assets/Palliative%20Care%20Community%20SQ%20policy%2028-Feb-2010_20120109162030.pdf.
Disclaimer: Source Accuracy
You are welcome to download and save a local copy of this document in the Word and/or PDF formats provided. As the POGO Satellite Manual is subject to ongoing revisions and updates by POGO, we recommend you regularly check the online version posted at https://www.pogo.ca/satellite-manual/ to ensure you have the most up-to-date content. In the event of any inconsistency between the content of a local copy and the online version of the POGO Satellite Manual, the content of the online version shall be considered correct. Please see also the POGO Satellite Manual Disclaimer.
Record of Updates
| Version Number | Date of Effect | Summary of Revisions |
| 1 | 6/28/2021 | Original version posted. |


{kind=link}